Die Infektionsrate von Covid-19 könnte bei Kindern, die eine Grippe-Impfung erhalten haben, um 440% höher sein und das während die Gesundheitsbehörden für die kommende Grippesaison mehr Impfungen fordern.
Eine neue Studie, die in der Fachzeitschrift Clinical Infectious Diseases veröffentlicht wurde, kommt zu dem Ergebnis, dass Kinder, die inaktivierte Grippeimpfstoffe erhielten, mit 440% höherer Wahrscheinlichkeit (relatives Risiko: 4,40; 95% Konfidenzintervall: 1,31-14,8) Infektionen mit respiratorischen Viruserregern, bei denen es sich nicht um Influenza handelt, bekamen.
Angesichts des aggressiven Drängens auf Influenza-Impfungen, das Aktuell propagiert wird, zeigt diese medizinische Empfehlung das Kinder möglicherweise extrem anfälliger für Coronavirus-Infektionen sind.
Die Studie mit dem Titel “Erhöhtes Risiko von Infektionen mit Nicht-Grippe-Respirationsviren in Verbindung mit dem Erhalt eines inaktivierten Grippeimpfstoffs” ist hier zu finden.
Die Studie kommt zu dem Ergebnis, dass Grippeimpfungen buchstäblich Teile des menschlichen Immunsystems inaktivieren, wodurch das Kind anfälliger für Coronavirusinfektionen wird. “Da sie gegen Grippe geschützt sind, kann es sein, dass dreiwertigen inaktivierten Grippeimpfstoffempfängern vorübergehend eine unspezifische Immunität fehlt, die vor anderen Atemwegsviren schützt”, schreiben die Autoren der Studie.
Die Studienautoren erklären, dass der Influenza-Impfstoff Influenzavirusinfektionen vorbeugt, gleichzeitig aber Kinder anfälliger für andere Atemwegsinfektionen macht. Da die Infektions-Todesrate (IFR) bei der saisonalen Grippe so niedrig ist (etwa 0,024%, was kein Tippfehler ist) und die Infektions-Todesrate bei Covid-19-Infektionen mindestens eine Größenordnung höher liegt, stellt sich die offensichtliche Frage:
Würde es demzufolge mehr Leben von Kindern retten, wenn sie dieses Jahr keine Grippeschutzimpfung bekämen und damit ihre Anfälligkeit für Covid-19, das eine weit höhere Sterblichkeitsrate aufweist, verringern?
Die Studie, die 2009 durchgeführt wurde, beobachtete die Ergebnisse von 115 Kindern im Alter von 6 bis 16 Jahren. Die Studie verwendete auch eine Placebogruppe und stellte fest, dass Placebo “keinen statistisch signifikanten Unterschied” im Risiko einer akuten Atemwegsinfektion macht.
Kinder, die gegen Grippe geimpft waren, hatten jedoch ein viel höheres Risiko für Atemwegsinfektionen.
Noch schockierender ist, dass die Studie auch keinen Unterschied im Risiko einer saisonalen Grippeinfektion zwischen den Kindern, die geimpft waren, und denen, die nicht geimpft waren, feststellte. Mit anderen Worten: Der Grippeimpfstoff bot keinen Schutz vor der Grippe, aber er erhöhte die Anfälligkeit für andere Atemwegsinfektionen. (Kein Nutzen, nur erhöhte Risiken.) “Es gab keinen statistisch signifikanten Unterschied im Risiko einer bestätigten saisonalen Grippeinfektion zwischen Empfängern von TIV oder Placebo”, erklärt die Studie.
A new study published in the journal Clinical Infectious Diseases finds that children who received inactivated influenza vaccines were 440% more likely (relative risk: 4.40; 95% confidence interval: 1.31-14.8) to acquire infections of respiratory viral pathogens which are not influenza. With the aggressive push for influenza immunizations now under way, the medical establishment may be setting up children to be extremely vulnerable to coronavirus infections.
Titled, “Increased Risk of Noninfluenza Respiratory Virus Infections Associated With Receipt of Inactivated Influenza Vaccine,” the study is found at this link at the National Library of Medicine: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3404712/
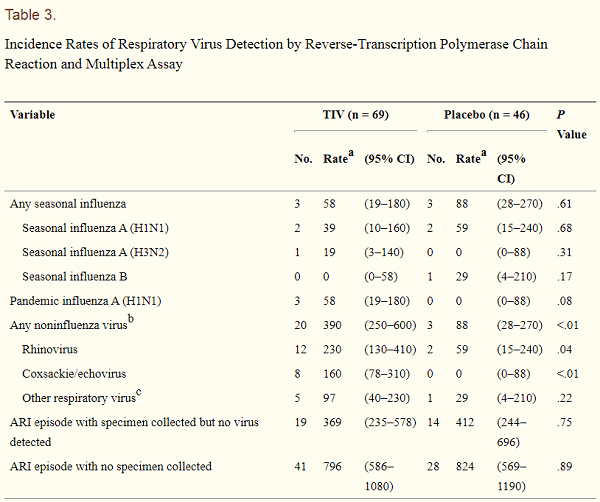
The study finds that flu shots quite literally inactivate parts of the human immune system, rendering the child more vulnerable to coronavirus infections. “Being protected against influenza, trivalent inactivated influenza vaccine recipients may lack temporary non-specific immunity that protected against other respiratory viruses,” the study authors write. The study authors explain that the influenza vaccine works to prevent influenza virus infections, but at the same time it makes children more susceptible to other respiratory infections. Since the Infection Fatality Rate (IFR) for seasonal influenza is so low (around 0.024%, which is not a typo), and the Infection Fatality Rate of covid-19 infections is at least one order of magnitude higher, it raises the obvious question: Would it save more lives of children to avoid administering flu shots this year and therefore reduce their vulnerability to covid-19, which has a far higher fatality rate? The study, which was conducted in 2009, observed the outcomes of 115 children aged 6 – 16 years. The study also used a placebo group and found that placebo made “no statistically significant difference” in the risk of acute respiratory infection risk. But children who received influenza vaccines had a much higher risk of respiratory infections. Even more shockingly,the study also found no difference in the risk of seasonal influenza infections between those children who were vaccinated vs. those who weren’t. In other words, the influenza vaccine offered no protection against the flu, but it created increased vulnerability to other respiratory infections. (No benefits, just increased risks.) “There was no statistically significant difference in the risk of confirmed seasonal influenza infection between recipients of TIV or placebo,” the study explains. You can see the increased number of respiratory infections in this chart. Note the “TIV” column means those children who were vaccinated with an influenza vaccine:
The conclusion is that influenza vaccines make children more susceptible to other respiratory viral infections. From the study, which took place more than a decade before the arrival of the covid-19 pandemic:
We identified a statistically significant increased risk of noninfluenza respiratory virus infection among TIV recipients (Table 3), including significant increases in the risk of rhinovirus and coxsackie/echovirus infection, which were most frequently detected in March 2009, immediately after the peak in seasonal influenza activity in February 2009.
The study authors point out that the influenza vaccine, “could increase influenza immunity at the expense of reduced immunity to noninfluenza respiratory viruses, by some unknown biological mechanism,” although they also state more research is needed because some of the self-reporting of symptoms may have introduced “artifacts” which could sway the numbers. Nevertheless, the study authors also state that this phenomenon of “viral interference” is well known:
Participants who received TIV would have been protected against influenza in February 2009 but then would not have had heightened nonspecific immunity in the following weeks… The phenomenon of virus interference has been well known in virology for >60 years [24–27]. Ecological studies have reported phenomena potentially explained by viral interference [3–11]… Interference in respiratory and gastrointestinal infections has been reported after receipt of live oral poliovirus vaccine [29–32].
Increased Risk of
Noninfluenza Respiratory Virus Infections Associated With Receipt of
Inactivated Influenza Vaccine
Clin Infect
Dis. 2012 Jun 15; 54(12): 1778–1783. Published
online 2012 Mar 15. doi: 10.1093/cid/cis307
Benjamin J. Cowling,1
Vicky J. Fang,1 Hiroshi Nishiura,1,2 Kwok-Hung Chan,3 Sophia Ng,1 Dennis K. M.
Ip,1 Susan S. Chiu,4 Gabriel M. Leung,1 and J. S. Malik Peiris1,5
1 School of Public
Health, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Pokfulam,
Hong Kong SAR, China; 2 PRESTO, Japan Science and Technology Agency, Saitama; 3
Department of Microbiology, Li Ka Shing Faculty of Medicine, The University of
Hong Kong, Queen Mary Hospital, 4 Department of Pediatrics and Adolescent
Medicine, The University of Hong Kong, Queen Mary Hospital, and 5 Centre for
Influenza Research, Li Ka Shing Faculty of Medicine, The University of Hong
Kong, Pokfulam, Hong Kong SAR, China
We randomized 115
children to trivalent inactivated influenza vaccine (TIV) or placebo. Over the
following 9 months, TIV recipients had an increased risk of
virologicallyconfirmed non-influenza infections (relative risk: 4.40; 95%
confidence interval: 1.31-14.8). Being protected against influenza, TIV
recipients may lack temporary non-specific immunity that protected against
other respiratory viruses
RESULTS
Among the 115
participants who were followed up, the median duration of follow-up was 272
days (interquartile range, 264–285 days), with no statistically significant
differences in age, sex, household size, or duration of follow-up between TIV
and placebo recipients (Table 1). We identified 134 ARI episodes, of which 49
met the more stringent FARI case definition. Illnesses occurred throughout the
study period (Supplementary Appendix Figure 1). There was no statistically
significant difference in the risk of ARI or FARI between participants who
received TIV and those who received placebo, either during winter or summer
2009 (Table 2). We were able to collect 73 NTSs for testing from participants
for 65 of 134 (49%) ARI episodes, which included 22 of 49 (45%) FARI episodes.
The mean delay between ARI onset and collection of first NTS was 1.22 days, and
5% of NTSs were collected >3 days after illness onset, with no statistically
significant differences between TIV and placebo recipients. We detected respiratory
viruses in 32 of 65 NTSs (49%) collected during ARI episodes, which included 12
of 22 (55%) FARI episodes. We collected 85 NTSs from participants at times when
one of their household contacts reported an acute URTI but the participants
were not ill, and identified viruses in 3 of the specimens (4%), including
influenza A (H3N2), coxsackie/echovirus, and coronavirus 229E. There was no
statistically significant difference in the risk of confirmed seasonal
influenza infection between recipients of TIV or placebo, although the point
estimate was consistent with protection in TIV recipients (relative risk [RR],
0.66; 95% confidence interval [CI], .13–3.27). TIV recipients had significantly
lower risk of seasonal influenza infection based on serologic evidence (Supplementary
Appendix). However, participants who received TIV had higher risk of ARI
associated with confirmed noninfluenza respiratory virus infection (RR, 4.40;
95% CI, 1.31–14.8). Including 2 additional confirmed infections when
participants did not report ARI, TIV recipients had higher risk of confirmed
noninfluenza respiratory virus infection (RR, 3.46; 95% CI, 1.19–10.1). The
majority of the noninfluenza respiratory virus detections were rhinoviruses and
coxsackie/echoviruses, and the increased risk among TIV recipients was also
statistically significant for these viruses (Table 3). Most respiratory virus
detections occurred in March 2009, shortly after a period of peak seasonal
influenza activity in February 2009 (Figure 1)